One bilingual record. Remote consultations and asynchronous follow-up that carry the same operational record as in-clinic care — for places where the nearest specialist is hours away.
Rural clinics, community-health posts, municipal networks, hospital telehealth, cross-border care programmes, and mobile field teams.
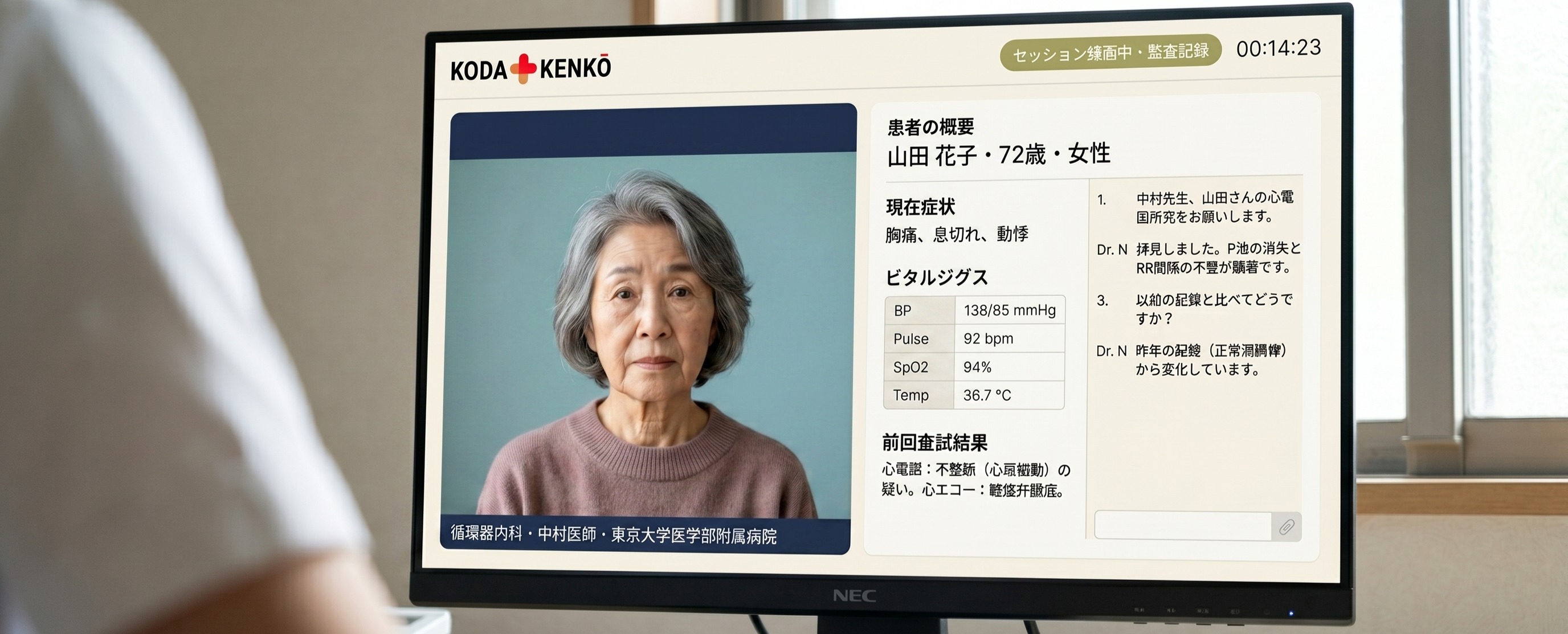
Clinician and specialist work from the same bilingual record — intake, vitals, SOAP draft, images, medication reference.
Nurse-led intake → case preparation → shared record → remote specialist → follow-up. End-to-end on the platform.
Foreign-patient intake in English, Portuguese, Chinese, Vietnamese, Tagalog, Nepali, and more. The local team uses the Japanese record; the specialist reads in their own language.
Every workflow is human-reviewed and logged in the audit trail. Clinic and specialist always read from the same record.
Nurse or clinician completes structured intake — vitals, symptoms, images, medication history, referral reason. The platform builds a bilingual case summary for specialist review.
Local clinic and remote specialist see the same context: SOAP structure, medication reference, prior encounters. Nothing lost in translation or hand-off.
The specialist reviews on their schedule. Comments, recommendations, and escalation flags enter the shared record — the local clinician sees them on the record they created. No phone tag, no lost faxes.
When a case needs immediate attention, the platform routes it to the on-call specialist with a priority flag and the full record attached — full context before they call back.
The platform translates the intake, organises the record, and routes the consultation. The local clinician reviews before sending; the specialist reviews before responding. Both decisions are recorded, the audit trail complete across every hand-off.
Reviewer, timestamp, and the content before and after review are all recorded. No clinical artefact enters the operational record without a qualified professional approving it.
The product does not consult, diagnose, or prescribe. It bridges the clinic to the specialist on a shared record so the people who do those things can do them with full context.
Telemedicine Bridge runs cloud-central with edge nodes at remote sites. The local team captures the case offline; it syncs to the specialist when connectivity returns. Built for Brazil’s rural and underserved regions; deployable wherever connectivity is unreliable or specialists are sparse.
Intake, SOAP, vitals, images, and medication reference structured for both clinic and specialist. Same record, two languages.
Specialists review on their schedule. Recommendations and escalations flow into the shared record — no phone tag, no lost faxes.
Priority cases routed to on-call specialists with the full record attached. Audit trail captures every escalation.
Edge nodes work without connectivity. Cases captured offline sync to the central platform when connection returns. Full audit history.
Cloud-central with edge nodes. Designed for Brazil’s rural regions; deployable anywhere specialists are sparse — Latin America, Southeast Asia, remote Japan.
20-minute walkthrough with KodaSōken engineering. We open a real case and run the remote consultation end-to-end on the shared bilingual record. No deck.